Influenza Update N° 421
Overview
13 June 2022, based on data up to 29 May 2022
Information in this report is categorized by influenza transmission zones, which are geographical groups of countries, areas or territories with similar influenza transmission patterns. For more information on influenza transmission zones, see the link below:
Influenza Transmission Zones (pdf, 659kb)
- The current influenza surveillance data should be interpreted with caution as the ongoing COVID-19 pandemic has influenced to varying extents health seeking behaviours, staffing/routines in sentinel sites, as well as testing priorities and capacities in Member States. Various hygiene and physical distancing measures implemented by Member States to reduce SARS-CoV-2 virus transmission have likely played a role in reducing influenza virus transmission.
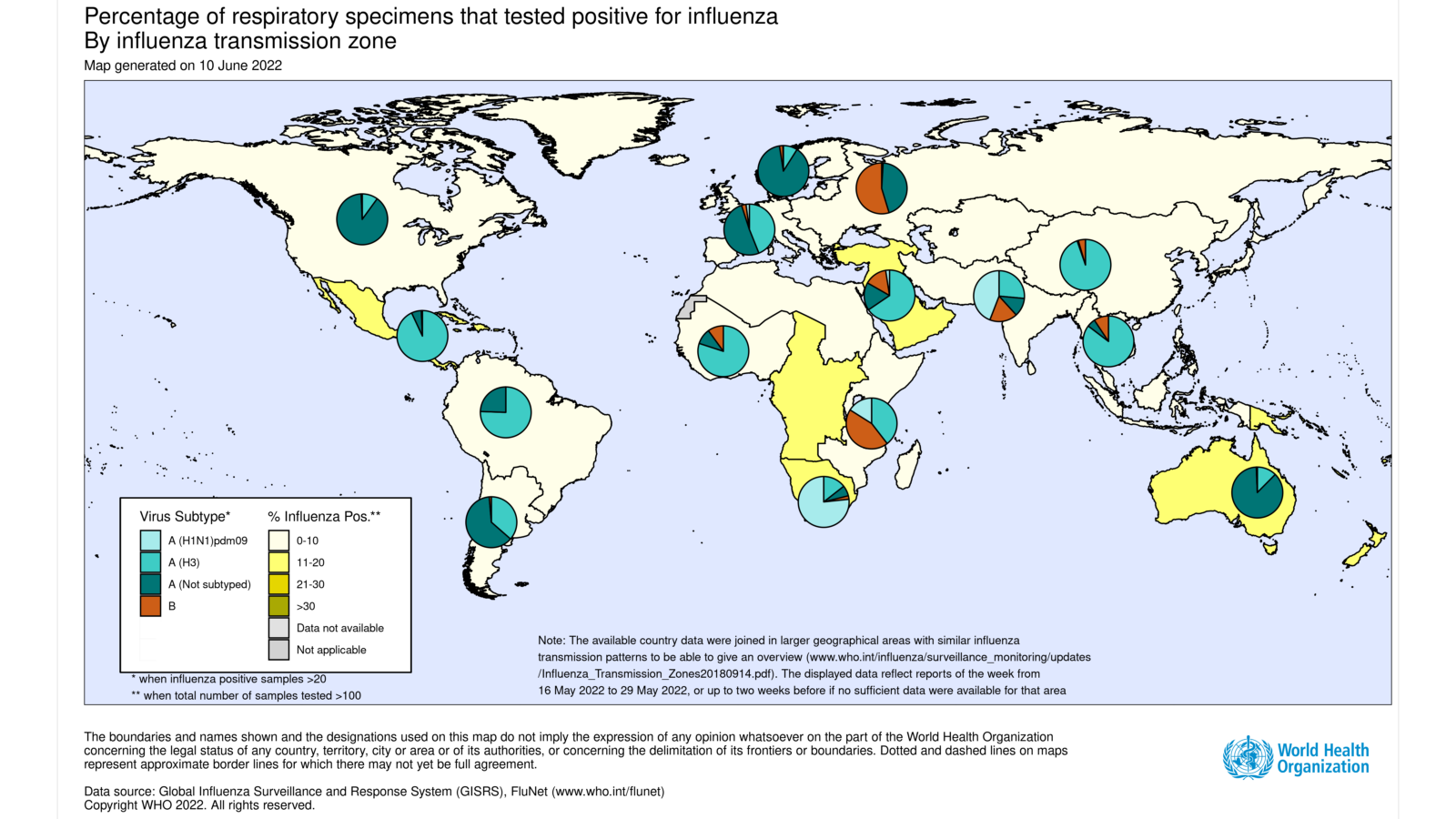
- Globally, influenza activity continued to decrease, following a peak in March 2022, but increasing activity in some areas of the temperate southern hemisphere has been reported.
- Countries are recommended to prepare for the co-circulation of influenza and SARS-CoV-2 viruses. They are encouraged to enhance integrated surveillance to monitor influenza and SARS-CoV-2 at the same time, and step-up their influenza vaccination campaign to prevent severe disease and hospitalizations associated with influenza. Clinicians should consider influenza in differential diagnosis, especially for high-risk groups for influenza, and test and treat according to national guidance.
- In the temperate zones of the southern hemisphere, overall influenza activity increased slightly in recent weeks.
- Detections of influenza A and respiratory syncytial virus (RSV) sharply increased in some regions of Australia.
- Influenza detections continued to increase in South Africa though the detections rate was at low levels.
- In temperate South America, influenza activity of predominately influenza A(H3N2) decreased in Argentina and Paraguay but increased in Chile and Uruguay.
- In the Caribbean and Central American countries, low influenza activity was reported with influenza A(H3N2) predominant.
- In tropical South America, low influenza activity was reported with influenza A(H3N2) most frequently detected followed by few influenza B viruses.
- In tropical Africa, influenza activity remained low with influenza A(H3N2) predominant.
- In Southern and South-East Asia, influenza virus detections were at low levels overall.
- In the countries of North America, influenza activity continued to gradually decrease compared to the previous period and influenza positivity was higher than usual for this time of year, compared to past seasonal influenza data reporting. Activity was predominantly due to influenza A viruses, with A(H3N2) predominant among the subtyped viruses. RSV activity remained low in Canada and the United States of America (USA).
- In Europe, overall influenza activity continues to decline with influenza A(H3N2) predominant among the subtyped viruses.
- In Central Asia, no influenza detections were reported.
- In Northern Africa, Tunisia reported a single influenza B detection.
- In Western Asia, increased influenza detections were reported in Qatar with influenza A(H3N2) most frequently detected.
- National Influenza Centres (NICs) and other national influenza laboratories from 112 countries, areas or territories reported data to FluNet for the time period from 16 May 2022 to 29 May 2022* (data as of 2022-06-10 08:29:54 UTC). The WHO GISRS laboratories tested more than 247 215 specimens during that time period. 14 614 were positive for influenza viruses, of which 14 322 (98%) were typed as influenza A and 292 (2%) as influenza B. Of the sub-typed influenza A viruses, 154 (4.4%) were influenza A(H1N1)pdm09 and 3311 (95.6%) were influenza A(H3N2). Of the characterized B viruses, 66 (100%) belonged to the B-Victoria lineage.
 During the COVID-19 pandemic, WHO encourages countries, especially those that have received the multiplex influenza and SARS-CoV-2 reagent kits from GISRS, to conduct integrated surveillance of influenza and SARS-CoV-2 and report epidemiological and laboratory information in a timely manner to established regional and global platforms. Revised interim guidance has just been published here: https://www.who.int/publications/i/item/WHO-2019-nCoV-integrated_sentinel_surveillance-2022.1.
During the COVID-19 pandemic, WHO encourages countries, especially those that have received the multiplex influenza and SARS-CoV-2 reagent kits from GISRS, to conduct integrated surveillance of influenza and SARS-CoV-2 and report epidemiological and laboratory information in a timely manner to established regional and global platforms. Revised interim guidance has just been published here: https://www.who.int/publications/i/item/WHO-2019-nCoV-integrated_sentinel_surveillance-2022.1.
- Overall COVID-19 positivity from sentinel surveillance increased during the reporting period to approximately 30%. The highest increases were observed in the Region of the Americas and the Western Pacific Region of WHO where positivity was around 20% and 30%, respectively. In the other Regions of WHO positivity was around or below 10%. Activity from non-sentinel sites was varied, with overall positivity around 15%.
- National Influenza Centres (NICs) and other national influenza laboratories from 44 countries, areas or territories from six WHO regions (African Region: 1; Region of the Americas: 16; Eastern Mediterranean Region: 4; European Region: 17; South-East Asia Region: 4; Western Pacific Region: 2 ) reported to FluNet from sentinel surveillance sites for time period from 16 May 2022 to 29 May 2022 (data as of 2022-06-10 08:29:54 UTC). The WHO GISRS laboratories tested more than 40 939 sentinel specimens during that time period and 7040 (17.2%) were positive for SARS-CoV-2. Additionally, more than 595 724 non-sentinel or undefined reporting source samples were tested in the same period and 99 461 were positive for SARS-CoV-2. Further details are included at the end of this update.
Source of data
______________________________________________________________________________________________
The Global Influenza Programme monitors influenza activity worldwide and publishes an update every two weeks. The updates are based on available epidemiological and virological data sources, including FluNet (reported by the WHO Global Influenza Surveillance and Response System), FluID (epidemiological data reported by national focal points) and influenza reports from WHO Regional Offices and Member States. Completeness can vary among updates due to availability and quality of data available at the time when the update is developed.
*It includes data only from countries reporting on positive and negative influenza specimens.