A young 27-year-old doctor working is incredulous about his low awareness about violence against women (VAW) despite treating survivors in the busy medical college hospital where he works in the western state of Maharashtra.
“I never looked at health complaints of female patients in the context of violence. I had no understanding about this issue. Now, I know what I should do, what should I say to make women comfortable,” said a doctor from District General Hospital, Sangli, in Maharashtra.
He and many other health care providers (HCPs) following a pilot training programme conducted in two medical colleges in between July 2018 and April 2019 on models of service delivery to provide women-centred response in line with WHO recommendations.

He is among 200+ HCPs trained in a mixed-methods implementation pilot to assess whether WHO clinical and policy guidelines to strengthen the capacity of health providers and improve health system readiness to respond to all forms of VAW are accessible, feasible, sustainable and effective.
Most HCPs are aware of their responsibility and with some training, become motivated agents of change. “We need to listen to her (survivor’s) carefully and offer suggestions. By looking at the wound, we can easily tell if it is accidental or assault. If a woman is saying it is assault, we should build rapport and encourage her to speak,” said a female nurse (obstetrics and gynaecology), from the Government Medical College and Hospital, Miraj, in Maharashtra.
“We had no idea [of] where women should go. Then, through the resource directory, we came to know that there are protection officers, there are many services where women can get help. We can provide shelter to women who don’t want to go back to their home,” said a 29-year-old male medical officer (Emergency Department), the Government Medical College and Hospital, Aurangabad, Maharashtra.
Begin to end VAW
Support from first responders like them and partners has led to incremental gains in reducing violence against women, but more concerted effort is needed to protect women, girls and children against all forms of violence particularly interpersonal violence.
have experienced either physical or sexual violence by an intimate partner or non-partner in their lifetime. Yet, many don’t report the violence or seek support because of fear of retribution from the perpetuators or rejection from the family and community. Among the Member States of the WHO South-East Asia Region, at 35%, India has the third highest estimated prevalence of lifetime intimate partner violence (IPV) among ever-married/partnered women aged 15–49 years, compared to the global average of 27%.
A recent demographic health survey from India (2019-2020) shows that there has been a decline in physical and sexual violence in most states and union territories (National Family Health Survey-NFHS IV), but progress remains uneven and insubstantial. With the COVID-19 pandemic burdening health systems and weakening support systems, the need to address violence against women needs more attention now than ever before. Maharashtra is one of the five states that registered an increase in VAW, from 21% in 2015-2016 to 25% in 2019-20 (NFHS IV and V).
The WHO’s Department of Sexual and Reproductive Health and Research and the Human Reproduction Programme together with the WHO Country Office for India, commissioned the Centre for Health and Enquiry into Allied Themes (CEHAT) to work with the Government Medical College and Hospital, Miraj-Sangli, and Government Medical College and Hospital, Aurangabad. The study methodology, findings and impact are available here.
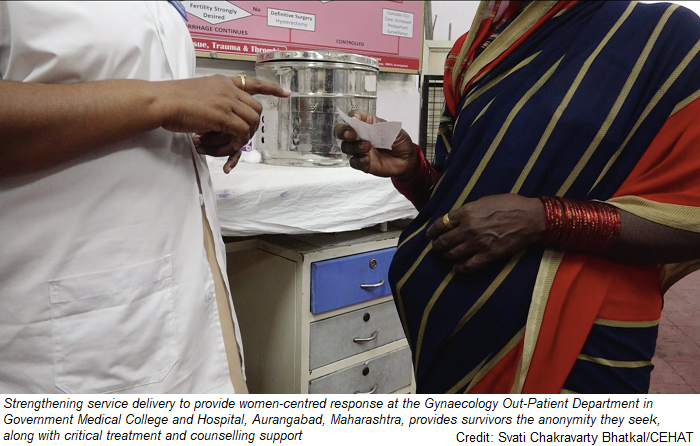
Strengthening service delivery to provide a woman-centred response in a clinical and health care settings provides survivors the anonymity they seek, along with treatment and counselling support.
“Such services should only be in hospital. Or mothers-in-law will ask, why you are going? What is the need to go? Mothers-in-law say such things. If we go to hospital, then such services should be there for us! The only place where we can go alone is the hospital…,” said a 20-year-old woman survivor who reported to one of the participating hospitals in the CEHAT study.
A sympathetic response encourages women to seek support without fear of being judged. “The doctor said come again if you feel like talking to me or need any help. She also shared her phone number. I felt there is someone who believes me and can guide me,” said another 32-year-old woman from the same group.
“I think it is important to train everyone. If there are providers who are not trained and are not sympathetic towards women, then the efforts which trained doctors are putting in will be in vain. There is no point in telling a woman that we are there to help her. She will not believe us because of her experience with untrained providers in the past,” said a male doctor.
Start of something big
“The quality of service I am providing has improved dramatically without my spending a single extra minute than before. I’d like hospital administrators to explain to our personnel how this (the training) is a quality addition without taking up more time… women have been encouraged to follow the legal procedure and have sought help and got redressal. Now, they bring other women with complaints, because they are assured of support and confidentiality at our facility, so it’s wonderful,” said Dr Pallavi Saple, Dean, Government Medical College, Miraj.
The pilot demonstrated that LIVES, the new standard first-line care recommended by WHO guidelines, can be implemented by health care providers with additional skill-based training and system-level action, particularly, at the facility-level. It found that it was critical to introduce health-system level changes before the implementation of the training intervention to create ownership through the engagement of managers and administrators.
While findings from the implementation research is a significant step towards better understanding the feasibility and application of WHO recommendations, it also highlights the system-level actions needed. In addition, targeting HCPs in planning, design and implementation with clear recognition of roles, responsibilities, constraints and barriers helped to keep motivation high. Full research brief is available here.
Young providers were more receptive to changes in attitudes as compared with older ones, underscoring the need for VAW in pre-service trainings. “Many women think that violence is a part of every woman’s life, so if we have posters which give information that violence is not acceptable under any circumstances, then it also encourages women to seek help,” said another doctor.
Partnering for change
The study was also done at a pivotal moment, just before the COVID-19 pandemic, that offered crucial opportunities for collaboration and partnerships that could be leveraged during health emergencies and humanitarian crisis. For India, the lessons from this study have served as an implementation guide to operationalise the health system response to VAW, as mandated by India’s National Health Policy (2017), with respect to the feasibility, acceptability, and sustainability of integrating the response into existing health services in the public health system.
It also served as a practical tool to identify the basic elements of a health system response to domestic violence and support the development of national protocols and training materials for HCPs to complement the national guidelines on medico-legal care for survivors of sexual violence.
The pilot study offers a pathway to incorporate the global plan of action to strengthen the role of the health system within a national multi-sectoral response to address interpersonal violence, particularly against women, girls and children.
“It is feasible to continue this training. The only thing it requires is for people to be sensitised properly and regularly monitored. So even if I am not there tomorrow, other people will take this over. So, when you ask, whose mindset has changed, I think I am the first example,” said Dr Shrinivas Gadappa, Head, Obstetrics and Gynaecology, Government Medical College and Hospital, Aurangabad, Maharashtra.