Hidden cities is a joint WHO / UN-HABITAT report about urbanization and global health issues. Photo stories from around the world reflect the hidden realities urban dwellers are facing, and highlight some health inequities.
Health equity
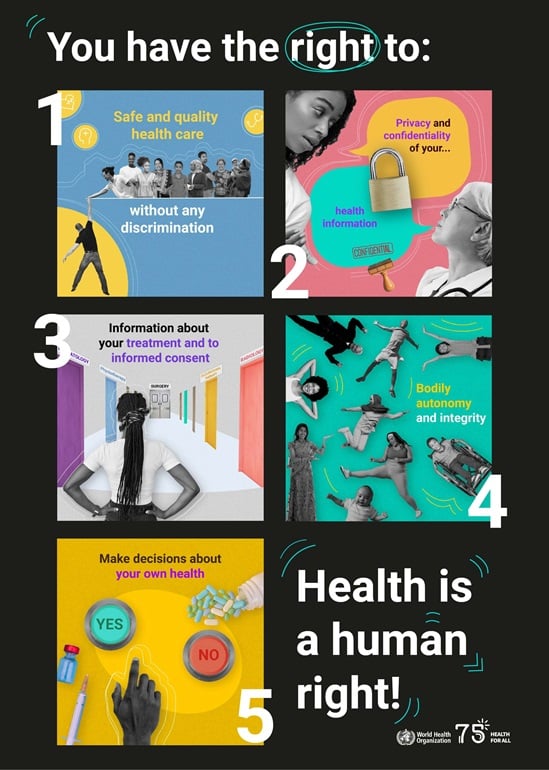
Equity is the absence of unfair, avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically or by other dimensions of inequality (e.g. sex, gender, ethnicity, disability, or sexual orientation). Health is a fundamental human right. Health equity is achieved when everyone can attain their full potential for health and well-being.
Health and health equity are determined by the conditions in which people are born, grow, live, work, play and age, as well as biological determinants. Structural determinants (political, legal, and economic) with social norms and institutional processes shape the distribution of power and resources determined by the conditions in which people are born, grow, live, work, play and age.
People’s living conditions are often made worse by discrimination, stereotyping, and prejudice based on sex, gender, age, race, ethnicity, or disability, among other factors. Discriminatory practices are often embedded in institutional and systems
processes, leading to groups being under-represented in decision-making at all levels or underserved.
Progressively realizing the right to health means systematically identifying and eliminating inequities resulting from differences in health and in overall living conditions.

Knowledge, monitoring, and analysis make up the backbone of actions needed to achieve equity. Monitoring health inequality must be central to a country’s health information system. This begins with the collection, analysis and reporting of data disaggregated by age, sex, education, income, disability and other factors. Qualitative data is also essential to understand the how and why of inequities. Data must also be linked with information on other determinants such as education to better understand cause-and-effect relationships i.e. how these other determinants contribute to health inequities. Part of inequality monitoring includes addressing gaps created by gender and other biases in how data has been previously collected, analysed and reported.
Equity, gender and rights-based assessment approaches and tools (including participatory approaches) should be used to systematically collect, collate, and analyze the evidence on health inequalities. This includes the health equity impacts of action by health and other sectors, for example reviewing specific aspects of the health system (e.g. Primary Health Care (PHC)/financing/health workforce) or of specific programmes (e.g. adolescent health/neglected tropical diseases/urban health). The findings need to be used to design responses for improved equity and ongoing monitoring of health inequalities.
To improve health equity, evidence-informed action is needed:
(1) by the health sector to ensure high-quality and effective services are available, accessible and acceptable to everyone, everywhere when they need them;
(2) by health and or other sectors to act on the wider structural determinants of health to tackle the inequitable distribution of power and resources, and to improve daily living conditions; and
(3) the health sector needs to take the lead in monitoring health inequities through monitoring health outcomes and health service delivery – as well as working with other sectors to monitor people’s living conditions.
Key examples include:
- redesigning health systems for equity e.g. pooling financial resources to enhance redistributive capacity and to progressively cover one billion additional people by 2023;
- prioritising the Primary Health Care approach e.g. investment of 1% of GDP in PHC;
- tackling structural determinants such as sexism, racism, ageism, classism and ablism;
- addressing harmful gender norms and gender inequalities in health policies/services/programmes and having more women in leadership positions and decision-making processes;
- protecting and increasing investment in health and other social sectors (through Universal Health Coverage (UHC), education and broader social protection) e.g. ensuring policies for decent work and employment conditions for all;
- ensuring equitable services and infrastructure in both urban and rural areas to ensure everyone can lead healthy lives; and
- continuing to monitor health inequalities and the impact of action.




/noncommunicable-diseases-rehabilitation-and-disability-(ncd)/sensory-functions-disability-and-rehabilitation-(sdr)/dg-video-message-for-international-day-of-persons-with-disabilities-2025.tmb-549v.jpg?sfvrsn=ae06296b_1)
/noncommunicable-diseases-rehabilitation-and-disability-(ncd)/sensory-functions-disability-and-rehabilitation-(sdr)/my-right.tmb-549v.jpg?sfvrsn=40e2dc7c_1)